Acne vs Pimples: Key Differences, Causes & Best Treatment
Confused between acne and pimples? Learn the key differences, root causes, and best treatments for glowing Indian skin in this expert guide.
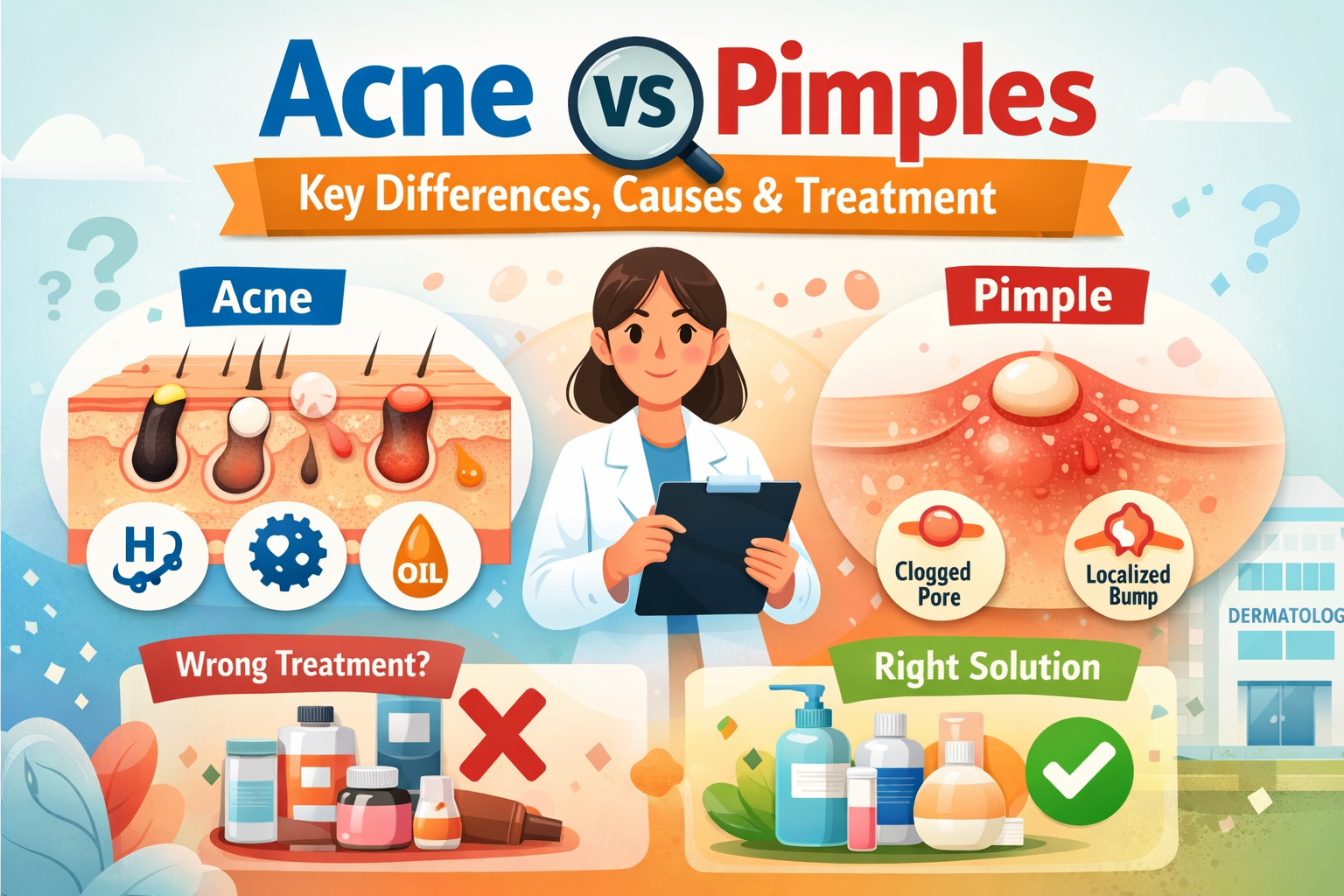
Acne vs Pimple at a Glanc
Acne is a long-term skin condition where different kinds of breakouts show up on the skin—like blackheads, whiteheads, cysts, and nodules. A pimple is just one small part of this condition. It’s that single, red, swollen, pus-filled bump you notice suddenly on your face. Simply put: every pimple is a type of acne, but acne is much more than just pimples.
If you’ve ever looked in the mirror and wondered, “Is this acne or just a pimple?”—you’re definitely not alone. At home, in WhatsApp chats, and even in beauty ads, these two words are often used as if they mean the same thing. But when it comes to choosing the right treatment, knowing the difference really matters.
Indian skin has its own set of challenges. The T-zone is usually oilier, dark spots after breakouts (hyperpigmentation) tend to stay longer, and hormonal changes from stress, diet, or conditions like PCOS can directly affect the skin. In this guide, we’ll break down the difference in a simple way, understand the causes, and talk about treatments that actually work well for Indian skin.
What Is Acne? In Complete Detail
Acne vulgaris—what we usually just call “acne”—is a long-term inflammatory skin condition that affects the pilosebaceous unit. That may sound technical, but the idea is simple: something goes wrong in the hair follicle and the oil (sebaceous) gland attached to it. When excess oil, dead skin cells, bacteria, and hormonal changes come together, acne develops.
This isn’t only a teenage problem. Dermatology research shows that around 85% of people between the ages of 12 and 24 experience acne at some point. But today, in cities like Mumbai, Delhi, and Bengaluru, adult acne is rising quickly among working women and men aged 25 to 35. Pollution, late-night stress, high-sugar diets (think refined flour, white rice, sugary tea), and hormonal imbalances related to PCOS are some of the key triggers for acne in Indian adults.
Acne is called a “condition” because it’s not just one bump that appears and disappears. It tends to come back repeatedly, shows up in different forms at the same time (blackheads on the nose, cysts along the jawline, papules on the cheeks), and often doesn’t clear up without proper treatment. That’s what makes it very different from a simple pimple
10 Best Dry Skin Foundation Tips In India
What Is a Pimple? Understand It Clearly
Clinically speaking, what we call a “pimple” is known as a papule (an inflamed bump without pus) or a pustule (a pus-filled bump). This happens when a clogged pore gets infected by Cutibacterium acnes (C. acnes). In response, your body sends white blood cells to fight the bacteria—and that reaction creates the familiar red, swollen bump, sometimes with a white tip, that we call a pimple.
Here’s something interesting: pimples can appear even in people who don’t technically have acne as a chronic condition. For example, someone might get one or two pimples around their period, or a bump on the forehead due to helmet friction. This doesn’t necessarily mean they have ongoing acne. That’s why treating occasional pimples and treating chronic acne with the same approach can be a mistake.
In many Indian households, the word “pimple” is used for almost any kind of bump on the face—whether it’s a whitehead, a cyst, or even milia (a small keratin-filled bump that isn’t caused by bacterial infection). Knowing the correct terms helps you communicate better with your dermatologist and choose the right skincare products for your skin.
Difference Between Acne and Pimple (Comparison Table)
| Feature | Acne | Pimple |
|---|---|---|
| Definition | Chronic inflammatory skin condition involving oil glands and pores | A single inflamed, pus-filled bump — one type of acne |
| Size / Spread | Multiple lesion types can appear together | One isolated lesion |
| Duration | Can last weeks to years; tends to recur | Often settles in 3–7 days |
| Causes | Hormones, bacteria, excess oil, dead cells, diet, pollution, stress | A blocked pore + bacterial infection |
| Types | Blackheads, whiteheads, papules, pustules, nodules, cysts | Papule (no pus) or pustule (with pus) |
| Severity | Ranges from mild to severe; clinically graded | Generally mild to moderate |
| Treatment | May need a dermatologist; long-term management | Often resolves on its own or with spot treatment |
| Dark Spots Risk | High — especially in darker Indian skin tones | Low — unless picked or popped |
In short: Every pimple is acne, but not every acne lesion is a pimple.
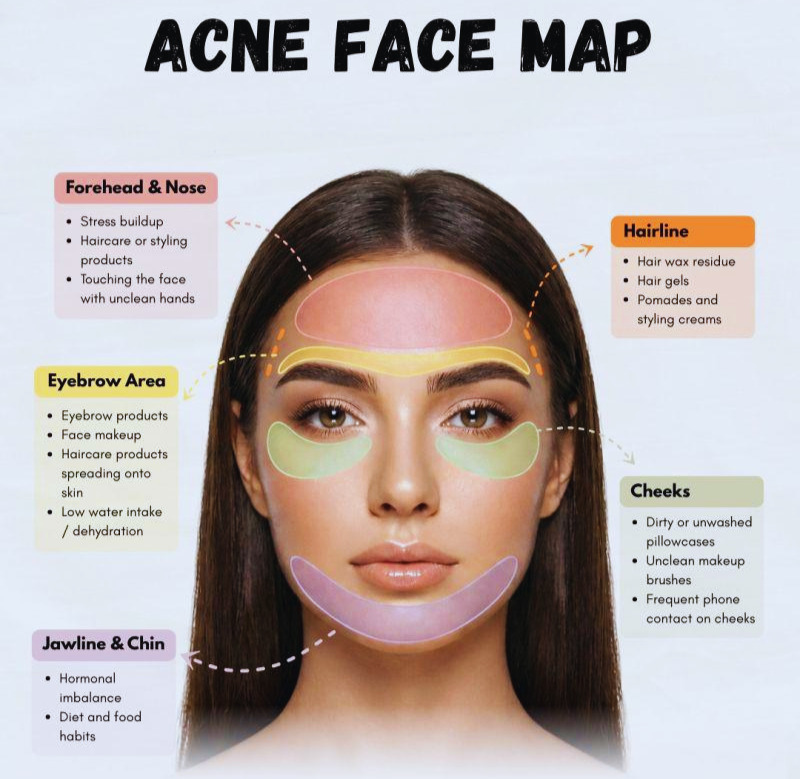
Why Does Acne Occur So Often in Indian Skin? — Root Causes

Acne and pimples rarely have a single cause. They are multi-layered, and triggers vary from person to person. However, certain factors are strongly linked with Indian skin types, climate, diet, and lifestyle. Understanding these helps you treat the root cause, not just the surface symptom.
1) Excess Sebum (Oil) Production
South Asian genetics often mean more active sebaceous (oil) glands. The T-zone (forehead, nose, chin) tends to be naturally oilier. When excess oil mixes with dead skin cells, pores get blocked — the first step toward acne.
In humid cities like Mumbai and Chennai, sweat worsens this clogging.
2) Overgrowth of Cutibacterium acnes
The bacterium Cutibacterium acnes normally lives on everyone’s skin. Trouble begins when a clogged pore creates an oxygen-poor space where it multiplies rapidly. Your immune system reacts, causing the red, painful bump we recognize as a pimple.
3) Hormonal Imbalances
Androgens (male hormones present in women too) increase oil production. In many Indian women, fluctuations due to Polycystic ovary syndrome, menstrual cycles, pregnancy, or thyroid issues are common.
This often appears as stubborn, painful breakouts along the jawline and chin that keep returning.
4) High-Glycaemic Diet
Refined flour (maida), white rice, sugary drinks, and biscuits spike blood sugar. This raises insulin, which stimulates androgens — and that boosts oil production. Everyday refined carbs can be a hidden acne trigger.
5) Stress — A Major Skin Trigger
Exam pressure, work deadlines, traffic, and financial stress raise cortisol levels. Cortisol signals adrenal glands to produce more androgens, increasing oiliness and breakouts.
Stress-related acne is extremely common among students, professionals, and new mothers.
6) Pollution and Sun Exposure
In cities like Delhi, Ahmedabad, and Mumbai, air pollution exposes skin to particulate matter that clogs pores and creates oxidative stress. Add strong year-round UV exposure, and acne becomes more inflamed while post-acne marks stay darker for longer.
7) Comedogenic Products
Some popular creams, heavy foundations, and even hair oils (applied near the hairline) can clog pores. This leads to pomade acne on the forehead and temples — common, but often overlooked.
How Many Types of Acne Are There?
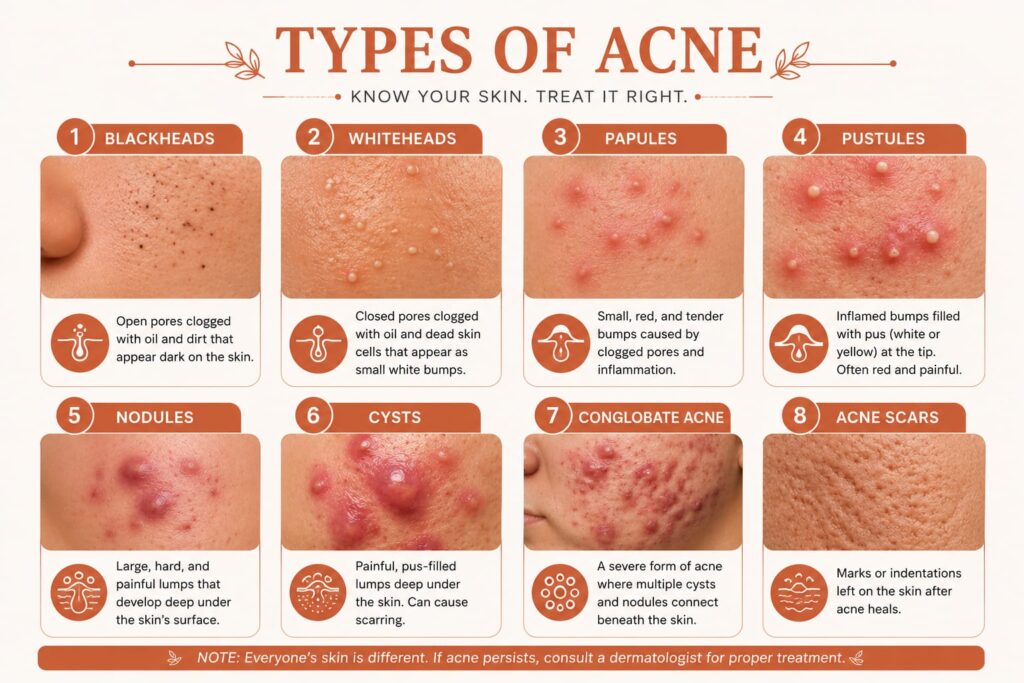
Before choosing a treatment, it’s essential to know exactly which type of acne you have. Each type forms through a different mechanism and responds to different ingredients. Misidentifying the type is one of the most common reasons treatments fail.
Blackheads (Open Comedones)
These are the small dark dots most commonly seen on the nose and chin. An important point: the dark color is not due to dirt. It’s oxidized sebum and melanin that turn dark when exposed to air. Blackheads are non-inflammatory and can usually be managed with a salicylic acid cleanser used regularly.
Whiteheads (Closed Comedones)
Similar to blackheads, but here the pore remains closed. Sebum and dead skin cells get trapped inside, forming a small white or skin-colored bump. They often appear in clusters on the forehead. AHA (such as glycolic acid) or retinoids work best for this type.
Papules
These are inflamed, raised, red bumps without a visible white head. This indicates that bacteria have triggered an immune response inside the pore. Never squeeze or pop a papule — this pushes bacteria deeper and significantly increases the risk of post-inflammatory hyperpigmentation (dark spots), especially in Indian skin tones.
Pustules (These Are “Pimples”)
The classic pimple — a red base with a white or yellow pus-filled tip. They are often painful to touch. Benzoyl peroxide spot treatment and a niacinamide serum can be helpful. However, in Indian skin, the dark spot left after healing (PIH) often lasts longer and appears more noticeable than the pimple itself.
Nodules
Large, hard, painful lumps deep under the skin. These cannot be popped and attempting to do so is dangerous. Nodular acne usually requires prescription treatment such as antibiotics or isotretinoin. If you experience nodules, consult a dermatologist rather than trying home remedies.
Cystic Acne
The most severe form of acne. These are large, soft, fluid-filled lumps deep within the skin. They are very painful, tend to recur in the same area, and carry the highest risk of scarring. Common on the jawline and cheeks and strongly linked to hormonal imbalance. This type requires medical treatment — no home remedy will be effective here.
Treatment: From Home Care to Clinic Care
Treatment exists on a spectrum — from gentle OTC products and evidence-backed home care to prescription medicines and in-clinic procedures. The right approach depends on your acne type, severity, and skin type. Here’s a structured breakdown.
OTC (No-Prescription) Treatments That Actually Work

Salicylic Acid (BHA) — 0.5% to 2%
Salicylic acid is oil-soluble, which means it can penetrate into the pore and dissolve sebum and dead cells. It’s ideal for blackheads, whiteheads, and mild inflammatory acne. Use daily in a face wash or toner.
Benzoyl Peroxide — 2.5% to 5%
One of the most effective OTC antibacterial ingredients — it directly kills C. acnes bacteria. Start with 2.5% to minimize dryness and irritation. It can bleach fabrics, so be careful. In hot weather, it may feel extra drying on Indian skin, so begin as a spot treatment.
Niacinamide (Vitamin B3) — 5% to 10%
This ingredient is especially beneficial for Indian skin. It regulates sebum production, minimizes the appearance of pores, reduces inflammation, and most importantly, helps fade post-acne dark spots (PIH). Gentle enough for daily use and highly recommended for acne-prone skin.
Retinoids (Retinol / Adapalene 0.1%)
Retinoids speed up cell turnover, prevent new comedones, and boost collagen production for acne scars. Adapalene 0.1% is available OTC. Start twice a week at night and always pair with sunscreen during the day. In the first 4–6 weeks, you may experience “purging,” where the skin appears worse before it improves — this is normal.
Azelaic Acid — 10% to 20%
An underrated multitasker for Indian skin. It targets bacteria, reduces inflammation, and treats pigmentation at the same time. It’s also pregnancy-safe and suitable for sensitive skin.
Prescription Treatments (Dermatologist Required)
Topical Antibiotics — Clindamycin, Erythromycin
Prescribed for moderate inflammatory acne to reduce bacterial load. Always combine with benzoyl peroxide to prevent antibiotic resistance. Avoid using these alone for longer than 3 months.
Oral Antibiotics — Doxycycline, Minocycline
Used for moderate-to-severe acne. Doxycycline is commonly prescribed. Take with food to avoid nausea and combine with a topical retinoid for best results.
Isotretinoin (Accutane / Roaccutane)
The most effective treatment for severe cystic or nodular acne. It can reduce sebum production by up to 80% and may lead to long-term remission. However, it requires monthly blood tests, strict sun protection, and mandatory contraception for women. Due to serious side effects, it must be taken only under dermatologist supervision.
Clinic Procedures That Show Visible Results

Chemical Peels (Glycolic, Salicylic, Mandelic)
Popular in dermatology clinics. Mandelic acid peels are often preferred for darker Indian skin tones because they carry a lower risk of post-peel hyperpigmentation. These peels deeply exfoliate, unclog pores, and help fade acne marks faster.
LED Light Therapy
Blue light targets C. acnes bacteria, while red light reduces inflammation and speeds up healing. Visible improvement is often seen in 6–8 sessions. It’s non-invasive, safe for all skin tones, and has no downtime.
Microneedling + PRP
Best suited for acne scars rather than active acne. Controlled micro-injuries stimulate collagen remodeling. When combined with PRP (Platelet-Rich Plasma), it shows significant improvement in atrophic (sunken) acne scars, especially in Indian skin.
Important Warning for Indian Skin
Treatment exists on a spectrum — from gentle OTC products and evidence-backed home care to prescription medicines and in-clinic procedures. The right approach depends on your acne type, severity, and skin type. Here’s a structured breakdown.
Daily Skincare Routine for Acne-Prone Indian Skin

Building a consistent, correct routine is the most important part of skincare. The goal is simple — clean without stripping, treat without irritating, and protect without clogging. Here’s a simple yet genuinely effective morning and night routine.
Morning Routine (Only 3 Minutes)
Gentle Foaming Cleanser (pH 4.5–5.5)
Use a sulphate-free, low-pH cleanser. One with salicylic acid or niacinamide is even better. Avoid soap — it disrupts the skin’s natural acid mantle and can actually increase oil production.
Niacinamide Serum (5–10%)
Apply 3–4 drops on damp skin. It’s perfect for daytime use — regulates sebum, soothes redness, and works on existing dark spots.
Lightweight, Non-Comedogenic Moisturiser
Choose a gel or lotion format with ingredients like hyaluronic acid or ceramides. Even oily skin needs moisturiser. Lack of hydration can trigger more oil production — one of the most common misconceptions.
Broad-Spectrum SPF 30–50 (Non-Comedogenic)
This is non-negotiable. UV exposure worsens acne inflammation and keeps post-acne marks darker for months. Use a mineral or hybrid sunscreen formulated for oily or acne-prone skin.
Night Routine

Oil Cleanser or Micellar Water (Double Cleanse)
First, remove sunscreen, pollution, and makeup without rubbing the skin. An oil cleanser does not cause acne — it actually dissolves excess sebum effectively.
Gentle Foaming Cleanser (Same as Morning)
Follow with a water-based cleanser to ensure no residue is left behind.
Treatment Active (Retinoid OR BHA Toner — Alternate)
Use a retinoid (like adapalene 0.1%) three nights a week. On the other nights, use a BHA toner. Do not use both on the same night — this can over-exfoliate the skin and damage the barrier.
Moisturiser (Slightly Richer Than Morning)
At night, the skin goes into repair mode. A slightly more nourishing moisturiser supports the skin barrier, especially when using retinoids.
You can also try 5 homemade face packs for glowing skin summer for fresh and healthy skin
Biggest Myths About Acne — Busted!
Myth vs. Science
In Indian households, you hear many things about acne that are not only incorrect but can actually make the skin worse. Let’s break the most common myths — with the help of science.
Common Myths About Acne
Myth: Oily or fried food causes pimples
Partially false. A pimple does not appear on your face right after eating cheesy pizza — that’s not how the mechanism works. High-glycaemic foods (sugar, refined flour) can worsen acne, but they act through hormonal pathways, not by directly clogging pores. Eating oily snacks does not make your face oily in the way people assume.
Myth: Washing your face many times will cure acne
The opposite happens. Using a cleanser 3–4 times a day strips the skin’s protective acid mantle and disrupts the natural microbiome. This leads to rebound oil production and worsening acne. Washing your face twice a day — morning and night — is sufficient.
Myth: Apply toothpaste on a pimple overnight
Toothpaste contains fluoride, sodium lauryl sulphate, and mint, which can chemically burn the skin. This increases the risk of redness, dryness, and post-inflammatory hyperpigmentation (dark spots), especially in Indian skin. There is no scientific evidence that toothpaste helps pimples. Avoid this practice.
Myth: Sitting in the sun dries out acne
This is a dangerous myth. You may see temporary improvement, but UV radiation increases inflammation, keeps post-acne marks darker for months, and can even trigger new comedones. Always wear sunscreen — even if you are staying indoors.
Myth: Acne only happens to teenagers
Not true. Dermatologists in Indian metro cities report a significant rise in adult acne cases among people aged 25–40, especially women dealing with hormonal issues, stress, and processed food diets.
Frequently Asked Questions (FAQs)
Are pimples and acne the same thing?
No. A pimple is one type of acne — specifically a single inflamed, pus-filled bump. Acne is a chronic skin condition that includes multiple types of lesions such as blackheads, whiteheads, cysts, and nodules occurring together. Every pimple is a form of acne, but acne is not limited to pimples.
Can I get a pimple without having acne?
Yes. Stress, friction, comedogenic products, or hormonal shifts can cause one or two pimples even if a person does not have chronic acne. If breakouts are isolated, occasional, and heal completely, it is not considered clinical acne.
Why do dark spots remain after a pimple heals on Indian skin?
This is called post-inflammatory hyperpigmentation (PIH). In response to inflammation, the skin produces excess melanin. Indian skin (Fitzpatrick Types IV–VI) has more active melanocytes, so these dark marks last longer compared to lighter skin tones. Sunscreen, niacinamide, and azelaic acid are highly effective in preventing and treating PIH.
How long does it take to see results from acne treatment?
Topical treatments usually take 8–12 weeks of consistent use to show visible results. With retinoids, the first 4–6 weeks may involve “purging,” where the skin appears worse before it improves. Prescription or clinical treatments may show faster results. Patience and consistency are key — expecting results within a week is unrealistic.
When should I visit a dermatologist?
You should consult a dermatologist if you have nodules or cysts, if there is no improvement after 3 months of consistent OTC treatment, if scarring is occurring, or if acne is affecting your mental health and confidence. Early professional help can prevent permanent scarring and hyperpigmentation.
Conclusion
Understanding the difference between acne and pimples is essential for healthy skin. It helps you stop guessing and start treating your skin correctly. When you clearly know whether you are dealing with a simple pimple or a deeper acne condition, you can choose the right products, avoid harsh treatments, and prevent unnecessary skin damage.
Healthy, clear skin doesn’t happen overnight, but with the right knowledge and daily care, it becomes achievable and long-lasting.

 Admin
Admin
[…] Read this: Acne vs Pimples: Key Differences, Causes & Best Treatment […]
[…] Read this: Acne vs Pimples: Key Differences, Causes & Best Treatment […]
[…] Read this: Acne vs Pimples: Key Differences, Causes & Best Treatment […]
[…] Read this: Acne vs Pimples: Key Differences, Causes & Best Treatment […]
[…] Acne vs Pimples: Key Differences, Causes & Best Treatment […]
[…] Acne vs Pimples Difference. […]
[…] Oily skin can often lead breakouts, so read our Acne vs Pimples:Key Differences, Causes & Best T… […]